The story of former Leonard Davis Institute of Health Economics’ Executive Director William Pierskalla begins with his receipt of a Stanford University PhD in industrial operations research in 1965—the same year Medicare and Medicaid were signed into law.
For the first half dozen years of his career, Pierskalla, a systems engineer specializing in mathematical programming and inventory control, conducted research in areas like schedule planning for suburban railways, logistical systems for maintenance parts, and ordering policies for perishable products.
But then, a single phone call lured the early mainframe computer expert into a different area of interest where he would go on to ultimately head a unique health services research center at the University of Pennsylvania as well as become a key player in the creation of what would become the country’s most important health services research organization.
Nurse scheduling software
That career-changing call came from a colleague who was attempting to design an automated nurse scheduling system for large hospitals and asked for Pierskalla’s technical assistance. During the next six months, he collected and fed huge amounts of data into a punch-card computer system in a project that created a software system that scheduled thousands of nurses in hospitals across the U.S. and Canada.
Much of the work kept Pierskalla inside hospitals, interacting with nurses and analyzing their hour-to-hour working environment. One of the things he quickly noticed was that, in terms of inventory management of short shelf-life products, human blood was as perishable as it gets.
“Blood. That’s what hooked me into healthcare,” said Pierskalla.
After that initial hospital project ended, he won a federal grant to study blood supply policy and throughout the 70’s evolved into an oft-quoted national authority on blood banking practices. Now retired, the 81-year-old splits his time between a home in Florida and a lakeside cabin in northern Minnesota.
As part of its 50th Anniversary celebration in 2017, LDI is profiling its former Executive Directors. As LDI’s third chief from 1978 to 1983, Pierskalla oversaw a distinctly different period in which the Institute functioned as the federal government’s National Health Care Management Center (NHCMC). It was a time when Jimmy Carter was President and the previously tiny ranks of federal healthcare officials had burgeoned into a massive network of agencies charged with running what had become the world’s most expensive government-funded healthcare programs.
One rising trend throughout that bureaucracy—and the Congress that funded it—was a growing interest in how the emerging new field of academic health services research might be harnessed to the management and regulation of the massively complex and costly new Medicare and Medicaid programs.
In many ways, the story of William Pierskalla’s LDI is a chapter in the history of health services research itself—and the many permutations that field went through as practitioners and federal clients alike struggled to define exactly how such a discipline should fit and be funded within the American system of healthcare.
~ ~ ~
Although small numbers of scientists had taken an interest in studying logistical aspects of their era’s medical delivery systems since the early 1900s, the modern version of what became known as “health services research” dates to the early 1960s.
At the 1962 conference that for the first time drew together the small group of scientists then involved in the movement, Harvard’s Mary Lee Ingbar, PhD, MPH, described the challenge: “Despite its size and its astounding recent growth, amazingly little is known about the health industry as an economic system. Cost relationships cannot be pictured. Key variables cannot be identified. Economies of scale cannot be sharply defined. In consequence, guidelines for policy cannot be established,” she said.


As the LBJ Administration prepared to sign the Medicare/Medicaid legislation into law, early health services researchers warned that “guidelines for policy cannot be established” because “amazingly little is known about the health industry as an economic system.”
As the LBJ Administration and Congress moved toward their historic creation of Medicare and Medicaid in 1965, the same issues became a central concern. A NIH history paper would later look back at how those federal officials were abruptly forced to realize that the “management of the highly diverse and interdependent personnel, facilities and technologies that constitute modern healthcare institutions requires information similar to that employed by other complex business enterprises… the growing involvement of government in the financing, planning, and regulation of healthcare heightened the demand of government officials for knowledge to guide the formulation and implementation of policy.”
In 1966, as Medicare began signing up its first round of clients, the “health services research” field of scientific inquiry was officially recognized by the federal government when the NIH created a health services research section charged with reviewing grant proposals.
Meanwhile, the healthcare insurance industry was similarly recognizing the disruptions and new realities presaged by the launch of Medicare and Medicaid. In Philadelphia in 1967, these concerns were the driving force behind the University of Pennsylvania Wharton School’s decision to partner with insurance magnate Leonard Davis to create the country’s first academic center dedicated to interdisciplinary health services and policy research: the Leonard Davis Institute of Health Economics (LDI).
Two years later, in a richly funded and expansive embrace of the new field, Congress established the National Center for Health Services Research (NCHSR) within the Department of Health, Education and Welfare (HEW). During the next ten years, the number of scientists drawn to health services research swelled. At the same time, their investigative capabilities were steadily enhanced by advances in computer technology and the successful application of econometric methodologies to the unique complexities of the healthcare business.
But then, the science of health services research found itself bumping up against the political conflict inherent in both federal bureaucracy and the capital’s community of high-powered lobbyists determined to bend healthcare policymaking to their own ends.
~ ~ ~
From 1970 to 1978, as his studies of blood banking systems made him a nationally renowned figure in that field, health services researcher William Pierskalla was also a professor of industrial engineering and management science at Northwestern University in Illinois. There, he served as acting director of Northwestern’s newly organized Health Services Research Center.
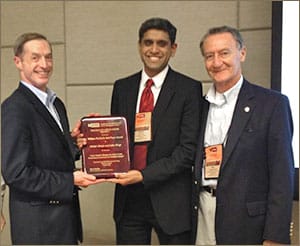
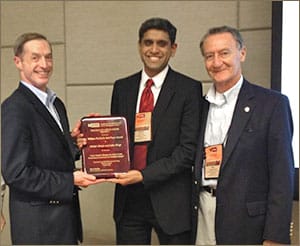
Throughout his 52-year career, Pierskalla has been a major presence in the international Institute for Operations Research and the Management Sciences (INFORMS). Here, in 2012, he officiates at the presentation of the annual INFORMS researcher award named in his honor: The Pierskalla Best Paper Award in Health Applications.
Two of his close colleagues in that research hub were whiz-kid health economist Mark Pauly, PhD, and Edward Hughes, MD, MPH, a Professor of Management Strategy, who Pierskalla brought in to become the center’s permanent director.
During the same period, Pierskalla was a rising star in the Operations Research Society of America [later to become the Institute for Operations Research and the Management Sciences (INFORMS)]. That scientific association focused on basic and applied research in the areas of industrial operational processes, decision-making and management science. By the second half of the 70s, Pierskalla was an executive committee member as well as the secretary of the organization; shortly thereafter he went on to become that organization’s president and later the president of the global International Federation of Operational Research Societies (IFORS).
This same systems engineering expertise would also give him an edge in the late 1970s’ world of health services research, which was being envisioned in new ways by federal grant sources.
~ ~ ~
In 1976, after ten years of Medicare and Medicaid operations, U.S. healthcare expenditures had risen 42% from 5.7% to 8.1% of GDP and, to the frustration of the Ford Administration and its Congress, showed no signs of slowing.
An IOM historical analysis of this same period noted a growing “sense of disappointment” throughout the Washington policymaking establishment “in the usefulness of the product of health services research.”
The IOM report faulted those policymakers for “unrealistic expectations” about identifying “quick fixes” to massively complicated problems but also emphasized that new measures were needed to learn more “about the complex variety of factors affecting our healthcare system.”
Basic research vs. applied research
In some D.C. policymaking circles this sense of frustration gave rise to the idea that health services research should not be viewed as an endeavor of “basic research” but rather as an “applied research” service in which scientists functioned as insightful consultants supporting the daily operations of healthcare industry managers.
“Basic research” as traditionally practiced in academia, refers to the scientific exploration of a problem without regard to any immediate commercial goal or use. “Applied research,” on the other hand, is scientific inquiry conducted to address a specific short-term commercial or societal objective.
This latter concept soon became the vision of how the potential cost-saving benefits of interdisciplinary health services research might be made more available to institutional and industrial managers. HEW’s new National Center for Health Services Research (NCHSR) created five new national health services research centers. Anchored in academia, each one was funded for five years and focused on different aspects of healthcare. Penn’s Leonard Davis Institute received $4.9 million (equal to about $20 million in 2016 dollars) to create and run the country’s first National Health Care Management Center (NHCMC).
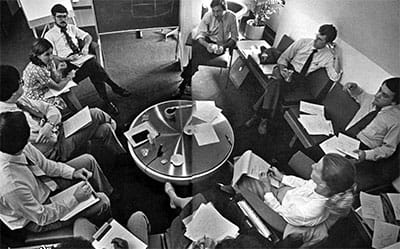
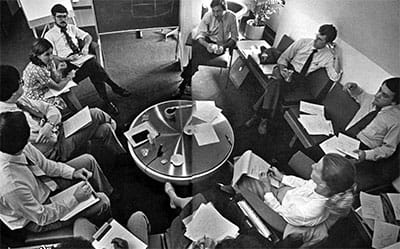
William Pierskalla (top, center) in a 1979 meeting with staff members of the new National Health Care Management Center (NHCMC) in LDI’s office building.
That NHCMC grant win was the largest amount of research funding yet received by the nine-year-old institute and made LDI a federal “special emphasis center” operating on a national scale.
The journal Health Affairs heralded the new center’s creation as an event of historical importance and said it would be “aimed at solving critical management problems in the nation’s healthcare delivery system.” Extensively quoted in the same article was LDI’s second Executive Director, Wharton and Medical School Professor Samuel P. Martin III, MD. He explained that it would be “extremely important” to keep activities of the new LDI center’s researchers “relevant to actual problems.”
One of the first things Martin did after securing the NHCMC grant was begin a search for a new faculty hire who had the qualifications and experience to organize and run a center focused on both healthcare delivery and practical applications research. Which is how operations and management expert William Pierskalla was lured from Northwestern University to Penn to simultaneously succeed Martin as LDI Executive Director and become Director of the new NHCMC.
Different philosophical vision
As he came on board in Philadelphia, Pierskalla joined with LDI Senior Fellow and Wharton Professor of Management Science John Hershey, PhD, to write a paper expressing a philosophical vision for the new national center that would become the core of LDI operations for five years.
They wrote, “We believe that Operations Research and Management Science can make major contributions to improving health services operations and national health policy…(and that) our profession must demonstrate greater capability and relevance.”
“We find it useful to distinguish between health services research and health services analysis,” they continued. “Health services research usually involves original investigation into specific problems associated with health services delivery using primary data collection and is relatively long-term. Health services analysis, on the other hand, is generally carried out in response to immediate problems faced by government decision-makers, regional planners, administrators, and providers. The analyst synthesizes existing research and data and must quickly summarize the advantages and disadvantages of alternative strategies for resolving problems.”
Pierskalla remembers that the idea of providing practical applications consulting services was not embraced by all LDI Senior Fellows.
“We had faculty and other people who didn’t want to do that kind of thing because they felt it was not academic,” Pierskalla said. “But there were enough people in leadership positions, like John Eisenberg, who wanted to reach out and solve problems and who helped to make it happen.”
More than 900 client projects
The resulting NHCMC era was one in which LDI largely veered away from basic academic research and put much more of its newly expanded resources into executive education and technical assistance services. From 1978 to 1982 the Center’s technical assistance department logged more than 900 different client projects for hospitals, HMOs, nursing homes, government agencies, labor unions and trade associations.
Asked to describe a typical project, Pierskalla detailed one focused on the fact that although West Virginia was one of the country’s poorest states with a chronic shortage of physicians, it simultaneously had the second highest level of per capita spending on medical education. Government officials there wanted to know why that was happening and how those costs could be brought into line. The Penn team’s analysis resulted in the Board of Regents of the Medical Schools changing the organization and financing of the state’s medical education system.
“We sent a technical assistance team with William Kissick and some of our other top people down there to go through the whole training process in the state’s three medical schools,” Pierskalla said. “Basically, the system they had was educating physicians for other states. We found that West Virginia was spending all this money to create physicians but as soon as those new doctors finished their residencies, they were able to leave for jobs in Pennsylvania, New York, Ohio and other places.”

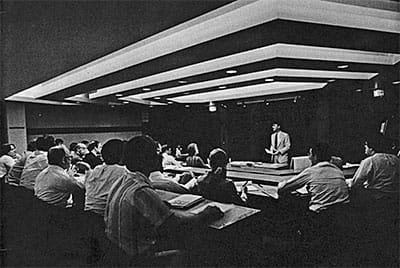
A 1979 National Health Care Management Center meeting of faculty senior fellows and staff held in LDI’s auditorium. During this period, the room on the ground floor of the LDI building was also the venue for executive education sessions attended by healthcare managers from across the country.
The Center’s technical assistance services also included the provision of one-to-three day on-site training seminars in clients’ locations across the country. Meanwhile, back in the LDI building on the Penn campus, the Center was providing executive education for HMO managers as well as other healthcare managers, planners and policy analysts. One of these groundbreaking training programs—for executive level nurses—drew the attention and then the long-term funding of Johnson & Johnson.
To better engage LDI Senior Fellows, the Center established a twice-monthly health service research seminar series for work-in-progress reports and peer comment. It also organized and managed six large-scale national conferences focused on practical application topics for healthcare managers across the country.
“When you walked into the LDI building in the morning, it was always buzzing,” said Joanne Levy, MBA, MCP, the then-research specialist who would later rise through the ranks to become LDI Deputy Director. “It was a whole different model from what LDI is today; we had project managers for technical assistance and executive education and research and there were always lots of different projects underway and members of various boards and the Center’s National Advisory Council were always marching in and out. And there was a large publishing operation. It took a lot longer to do things back then because we were still in the era of Selectric typewriters, cut-and-paste glue pots and mimeograph machines.”
Dissemination was a major mandate of the NHCMC grant; Pierskalla’s Center produced four different newsletters, including “INTERCHANGE” (a name later changed to “NHCMC Newsletter”), “UPDATE,” “Diagnostic Services Newsletter,” and “LDI News.” Working with LDI Senior Fellows, the communications staff also produced an “Issue Paper” series designed to provide problem-solving insights to health business managers, and “Discussion Papers” focused on faculty research results, policy analysis and the exploration of conceptual issues in health services research. It also published an ongoing “FACT PACK” series that provided practical application insights for problems common to large healthcare delivery system managers.
But then, as it moved through its fourth year, LDI and the other four centers originally created by HEW’s National Center for Health Services Research in 1977, were notified that their grants would not be renewed.
Over the fifteen years since both the HEW and Congress wholeheartedly embraced health services research as a crucial component of government healthcare management, there had been a change in attitudes. This was driven by the intensifying political battles surrounding healthcare spending as well as various sorts of intramural squabbling over control throughout the now sprawling federal healthcare bureaucracy.
Ironically, the closedown of the five centers run and staffed by the country’s top echelon of health services research leaders would give rise to a series of events that would ultimately re-invigorate and empower the profession as never before. LDI and William Pierskalla each played significant roles in this move that created the independent Association for Health Services Research (AHSR)—the national organization that would later change its name to AcademyHealth (Read the separate story: LDI and AcademyHealth).
~ ~ ~
Beyond running the National Health Care Management Center, Pierskalla greatly expanded the LDI/Wharton Health Care Systems Unit that, since 1967, merged the academic pursuits of both a leading medical and business school in a way that was nationally unique. But “units” in Wharton did not enjoy the same “seat at the table” privileges as departments, such as input in important school committees and faculty hiring authority. Pierskalla was determined to change this.


Pierskalla dramatically changed the Wharton School’s approach to healthcare management education when he succeeded in his campaign to upgrade healthcare management from a “unit” to a department with the ability to hire its own faculty and launch a PhD program.
“His greatest accomplishment during the period was his leadership in the conversion of that unit to a department and the creation of its PhD program,” remembered John Hershey, the Professor and LDI Senior Fellow who was then-director of the unit.
Pierskalla, who managed the PhD programs at Northwestern, recalled that “when I first arrived at Penn, LDI had no ability to hire faculty because they were only hired through a school department. My first goal was to convince Wharton to start a Health Care Management Department and launch a PhD program. In a research university like Penn, you had to have faculty and PhD students to support the full academic research process.”
Creating a new department within an Ivy League school is never an easy task, but Hershey said Pierskalla “demonstrated great political skill in overcoming resistance from many in Wharton to the idea that a department should be organized around an industry rather than a discipline or function.” He ultimately presented his proposal and supporting white paper to a full Wharton faculty meeting and won the vote by a large majority.
A second related educational accomplishment was Pierskalla’s recruitment of his former Northwestern colleague Mark Pauly to both lead the new PhD program and succeed him as executive director of LDI. The end result was a full-fledged nationally renowned Health Care Management Department that has since graduated more than 2,500 PhD and MBA graduates, many of whom have risen to top positions in academia, government agencies, healthcare organizations and industry.
After LDI, Pierskalla remained a Wharton Professor of Health Systems and Decision Science and became the school’s Deputy Dean for Academic Affairs. In a 1990 program for Project Hope in the wake of the collapse of the Soviet Union, he went to Europe to set up healthcare management training programs in Czechoslovakia, Hungary, Poland, Lithuania, Estonia and Latvia.
In 1993, Pierskalla was appointed Dean of the UCLA Anderson Graduate School of Management and continued his role as an international expert on blood banks and active past president of the Institute for Operations Research and Management Sciences (INFORM).
“Before coming to LDI,” said Pierskalla, “I had been working on things like blood banking and nurse scheduling, which were important but were micro issues. At LDI I had to look at macro issues from a systems engineering and management perspective. The whole interaction with multi-disciplinary groups was different and mastering that helped me a lot when I later moved into managing a business school. LDI had a huge impact on my research and the trajectory of my intellectual career. I really owe Penn a lot.”
Editor’s note: This post was originally published on the Leonard Davis Institute of Health Economics website as part of their eMagazine, the LDI Health Economist. View the original post here.